|
|
视网膜母细胞瘤(Retinoblastoma, Rb)俗称眼癌,是生长在视网膜上的恶性肿瘤,通常发病在3岁以下儿童,是婴幼儿常见的眼内恶性肿瘤,视网膜母细胞瘤的临床表现复杂,最常见的就是白瞳症,其他还有表现为结膜内充血、水肿、角膜水肿、虹膜新生血管、玻璃体混浊、眼压升高及斜视等。
首都医科大学北京儿童医院眼科赵军阳医生,在Ophthalmology发表的有关视网膜母细胞瘤玻切治疗的学术文章,该文章主要讲述了在治疗儿童视网膜母细胞瘤通过玻切手术后,对其近5年的预后随访数据的分析。
该文章参与的其他作者如下:
李琦炎医生,来自首都医科大学北京同仁医院眼科。
吴松一医生,来自泉州儿童医院眼科。
金丽文医生, 来自泉州儿童医院眼科。
马晓丽医生,来自首都医科大学北京儿童医院血液肿瘤中心
金眉医生, 来自首都医科大学北京儿童医院血液肿瘤中心
王一卓医生,来自首都医科大学北京同仁医院儿科。
BRENDA GALLIE医生,来自Departments of Ophthalmology & Vision Science, Hospital for Sick Children and University of Toronto, Toronto, Canada. Techna Institute, University Health Network, Toronto, Canada
Ophthalmology 为世界顶级的眼科学学术类网站,官方网址:https://www.aaojournal.org/
目前未做改文章的中文翻译,待时间充裕,我将对该文章进行翻译及数据分析解读,原文如下:
Pars Plana Vitrectomy andEndoresection of Refractory Intraocular Retinoblastoma
Unplannedintraocular surgery in eyes with active retinoblastoma carries a risk ofextraocular extension and metastases. Planned intravitreal chemotherapy (IVitC)has significantly revolutionized the treatment of the mostintractable feature of recurrent retino-blastoma, vitreous seeds, withoutevidence of extraocular spread of tumor. One child with recurrent refractoryvitreous seeding was treated with pars plana vitrectomy (PPV) with good visionand no active tumor at 26 months of follow-up.
We nowreport results of planned PPV and endoresection of active retinoblastomarefractory to standard treatments (systemic chemo-therapy, intra-arterialchemotherapy, focal therapy including brachy-therapy, and intravitrealmelphalan) in 21 children with only one remaining eye, as an alternative toenucleation (Fig 1). Institutional ethics review board approval was obtainedfrom Beijing Children’s Hospital and QuanzhouChildren’sHospital for this retrospective review of the medical records of childrentreated with PPV. A team approach included the retinoblastoma expert (J.Z.) whoindicated the intended target for PPV and expert retinal surgeons (Q.L., S.W.)who performed the PPV. The children were referred when retinoblastoma treatedin multiple institutions was unresponsive to standard therapies. All childrenhad no tumor obstructing visibility of the optic nerve or suggestion of nerveinvasion on neuroimaging and no evidence of extraocular disease at any time(before or after PPV).
BeforePPV, all children received a median of 6.5 cycles (range, 2-15 cycles) ofsystemic chemotherapy with carboplatin, etopo-side or teniposide, andvincristine (and cyclophosphamide for patients 5 and 14); 4 eyes experiencedretinal detachment (patients 3, 15, 16, and 17); 2 eyes (patients 11 and 21)received IVitC; 1 eye (patient 5) underwent brachytherapy with cataractextraction; and 3 eyes (patients 1, 11, and 20) received intra-arterialchemotherapy.
Three-portPPV was performed with a 23- or 25-gauge cutter probe with a nonvalved cannulawith 5 mg/ml melphalan in irrigation fluid. Alaser barrier around solid tumors and silicone oil stabilized the retina. Toreach anterior segment seeding (patient 4), the lens was removed and the tumorwas aspirated from the anterior chamber. Solid active tumor was removed byendoresection. After PPV, 0.2 ml melphalan (5 mg, 25 mg/ml) was injectedsubconjunctivally at surgical entry points and repeated at the subsequent 2-4examinations under anesthesia. Intravitreal chemotherapy (melphalan, 20 mg/0.05ml) was given monthly if extensive tumor had been removed (patients 8-17). Regularexaminations under anesthesia followed PPV.
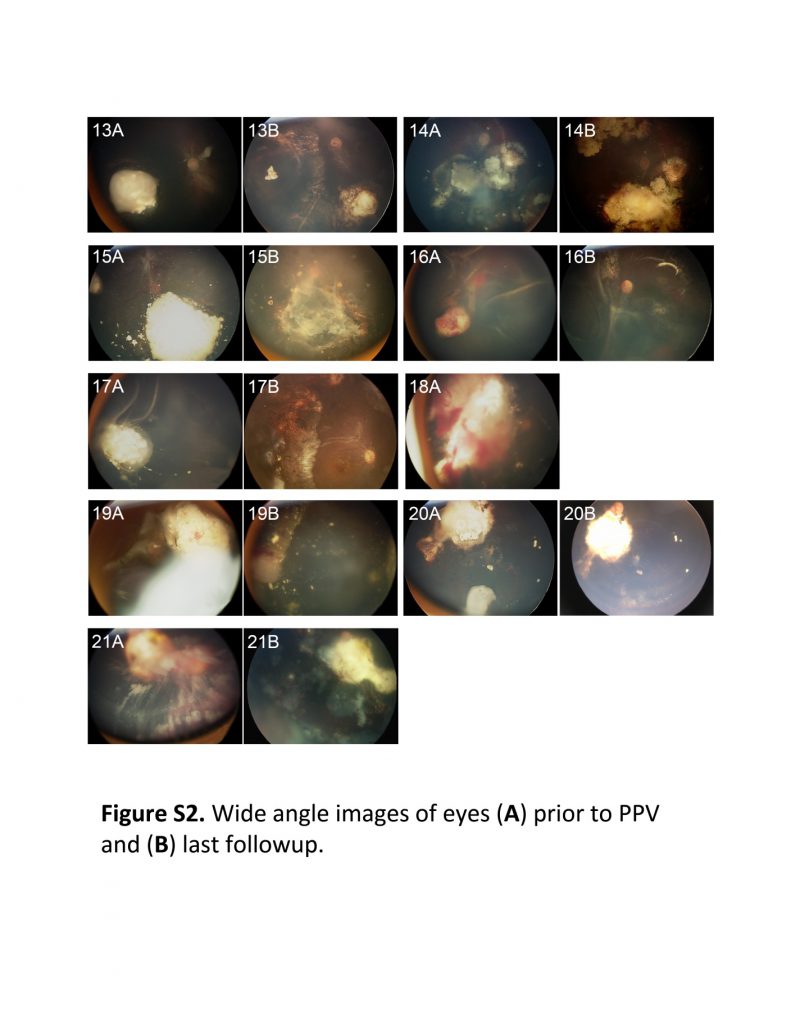
Up tothe end of 2016, follow-up time from diagnosis was a median of 5.1 years(range, 2.8-10.7 years); that from PPV was 3.3 years (1.6-4.3 years; Fig 1; FigS1). One patient (patient 21) was lost to follow-up with recurrent intra-oculartumor. As far as is known at this time, no patient demonstrated metastases ordied. Two eyes (patients 19 and 20) underwent enucleation for intraocular tumorrecurrence; 18 eyes were salvaged. Available wide-fieldretinal images of all 21 eyes before PPV and at last follow-up are shown in FigureS2.
Thelast follow-up visual acuity was functional in 14 of the 18 assessable salvagedeyes (78%; 11 had better than 20/80 vision; 2 had 20/100 vision; 1 had 20/200vision) and poor in 4 children (3 had counting fingersvision; 1 had light perception vision) (Fig S1).
AfterPPV, 5 patients required no more treatment (Fig 1A). Two patients (patients 4and 13) received 1 cycle of systemic chemotherapy because of suspectedchoroidal involvement at the resection site, and 2 because the other eye hadhigh risk pathology after enucleation (Fig 1B). One patient underwent surgeryfor retinal detachment (patient 17) and 2 patients underwent cataract surgery(patients 15 and 19). Ten patients with a high burden of vitreous seeds at PPVreceived adjuvant IVitC 1-4 times (Fig 1C). One patient (patient 18) receivedIVitC to treat residual vitreous seeds, but still required enucleation. Fourpatients (patients 12, 13, 16, and 17) received IVitC while silicone oil was inthe eye; no retinal toxicity was observed.
Theretinoblastoma was not controlled by 1 PPV in 4 patients, all of whomdemonstrated recurrence with difficult-to-visualizeanterior tumor (Fig 1D). Two patients underwent enucleation for recurrentdisease; no tumor was observed in the needle tracts on pathologic examination(patients 18 and 19). Two patients received 1 (patient 20) or 2 (patient 21)additional PPVs for recurrent tumor. Patient 20 achieved 20/100 vision after asecond PPV. The parents of patient 21 declined enucleation for recurrence after3 PPVs, and the child is now lost to follow-up.
Lastfollow-up vision (Fig 1; Fig S1) was functional in 14 of 18 assessable eyes(78%; 11 with better than 20/80 vision; 2 with 20/100 vision; and 1 with 20/200vision) and poor in 4 eyes (3 with counting fingers vision;1 with light perception vision). We observed no dissemination of cancer cellsoutside the eye at 3.3 years median follow-up after PPV.
Thelost-to-follow-up patient (patient 21) received 9 cycles of systemicchemotherapy, enucleation of the other eye, 4 IVitC injections, and 3 PPVs foranterior recurrent tumor that failed to control the cancer (Fig 1D; Fig S2).Enucleation was proposed repeatedly, but declined, and the child is lost tofollow-up with active intraocular disease. Unless treatment is ongoingelsewhere, this child may eventually die of recurrent retinoblastoma. Thelost-to-follow-up rate in China (2006-2008) was 40% at 5 years after diagnosis,currently estimated at 20% (J. Zhao, unpublished data, 2016), higher than thatof our present study (1/21 [5%]).
Organsalvage cancer therapy is common for most cancers, but the vastly differentsurvival rates for intraocular and extraocular retinoblastoma have dissuadedophthalmologists from exploring so-called lumpectomy for retinoblastoma. InChina from 2006 through 2009, 55% of children demonstrated advancedInterna-tional Intraocular Retinoblastoma Classification(IIRC) Group E retinoblastoma (enucleation recommended) and 33% demonstratedGroup C/D disease (considered safe to attempt salvage). Despite systemicchemotherapy, focal intra-arterial chemotherapy, or both, followed by focaltherapy (laser, cryotherapy, and IVitC), recurrence commonly leads to extensiveongoing treatments focused on saving the eye. This large investment may causeparents to resist enucleation when that becomes the safest option.
Thecareful approach developed by Munier et al for IVitC has no reported occurrenceof extraocular spread of tumor. For the many children in China with recurrentdisease after all standard therapies, a direct and definitivetherapy to save remaining eyes was needed: PPV and tumor resection achievedthis goal for 18 of 21 children with no instance of extraocular spread oftumor. This approach to retinoblastoma depends on multidisciplinary teamworkand careful technique to avoid tumor spread.
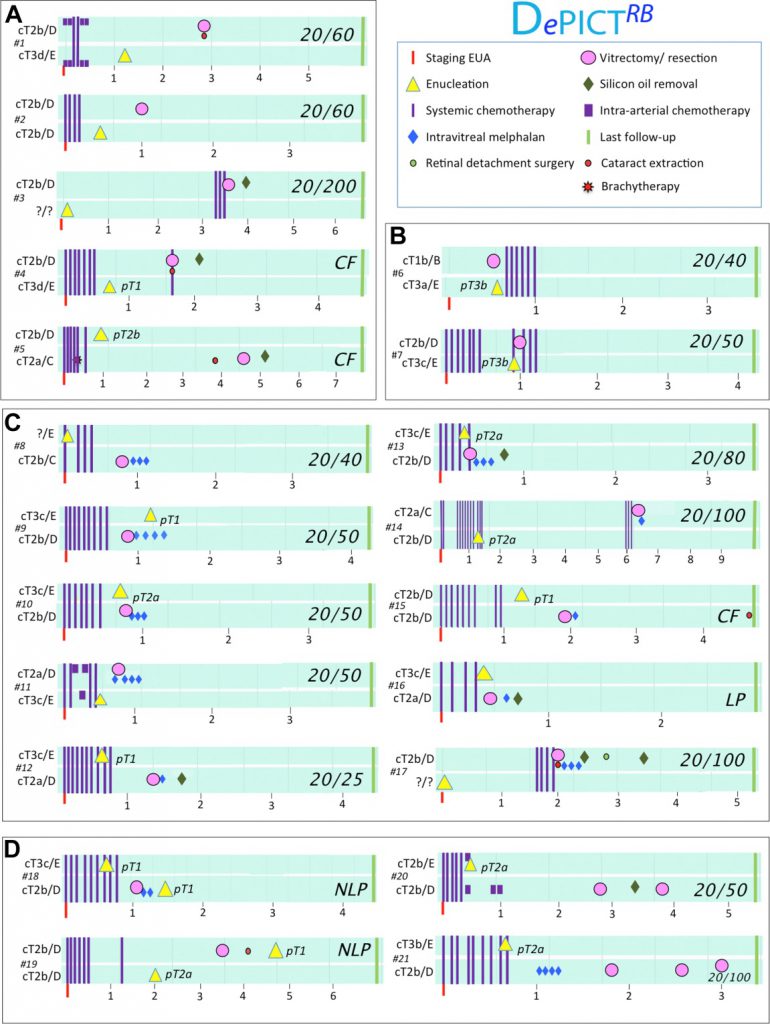 Figure 1.DePICTRB (Disease-specific, electronic Patient Illustrated ClinicalTimeline retinblastoma) summaries of children treated with pars planavit-rectomy (PPV). A, For 5 patients after PPV, no further treatments wererequired. B, Patients 6 and 7 were treated with systemic chemotherapy withcarboplatin, etoposide, and vincristine after PPV because of high-riskpathologic features in the enucleated eye. C, Ten patients were treated withintra-vitreal chemotherapy (IVitC) with melphalan after PPV. D, Four eyesfailed primary PPV: patients 18 and 19 underwent enucleation, a second PPVsaved patient 20 with 20/50 vision, and patient 21 remains lost-to-follow-upwith 20/100 vision after 2 subsequent PPVs. The follow-up from diagnosis andfrom PPV is displayed by the years between staging examination under anesthesia(EUA) and PPV and the right green line indicating last follow-up. Cancerstaging by International Intraocular Retinoblastoma Classification(IIRC) and the eighth edition of the American Joint Committee on Cancer StagingManual.5 Four patients (patients 4, 5, 14, and 21) had a family history ofretinoblastoma. CF ¼ counting fingers; NLP ¼ no lightperception. Figure 1.DePICTRB (Disease-specific, electronic Patient Illustrated ClinicalTimeline retinblastoma) summaries of children treated with pars planavit-rectomy (PPV). A, For 5 patients after PPV, no further treatments wererequired. B, Patients 6 and 7 were treated with systemic chemotherapy withcarboplatin, etoposide, and vincristine after PPV because of high-riskpathologic features in the enucleated eye. C, Ten patients were treated withintra-vitreal chemotherapy (IVitC) with melphalan after PPV. D, Four eyesfailed primary PPV: patients 18 and 19 underwent enucleation, a second PPVsaved patient 20 with 20/50 vision, and patient 21 remains lost-to-follow-upwith 20/100 vision after 2 subsequent PPVs. The follow-up from diagnosis andfrom PPV is displayed by the years between staging examination under anesthesia(EUA) and PPV and the right green line indicating last follow-up. Cancerstaging by International Intraocular Retinoblastoma Classification(IIRC) and the eighth edition of the American Joint Committee on Cancer StagingManual.5 Four patients (patients 4, 5, 14, and 21) had a family history ofretinoblastoma. CF ¼ counting fingers; NLP ¼ no lightperception.
   Acknowledgments Acknowledgments
Theauthors thank Ivana Ristevski for data analysis and figuredevelopment; Cynthia Vandenhoven, Raumil Patel, and Kaitlyn Hougham for figuredevelopment; and Sameh Soliman for manu-script review.
1.JUNYANGZHAO, MD
2.QIYANLI, MD
3.SONGYIWU, MD
4.LIWENJIN, MD
5.XIAOLIMA, MD
6.MEIJIN, MD
7.YIZHUOWANG, MD
8.BRENDAGALLIE, MD
1. Departmentof Ophthalmology, Beijing Children’s Hospital, Capital MedicalUniversity, Beijing, China.
2.Departmentof Ophthalmology, Beijing Tongren Hospital, Capital Medical University,Beijing, China.
3.Departmentof Ophthalmology, Quanzhou Children’sHospital, Quanzhou, China.
4.Departmentof Ophthalmology, Quanzhou Children’sHospital, Quanzhou, China.
5.Hematologyand Oncology Centre, Beijing Children’sHospital, Capital Medical University, Beijing, China.
6.Hematologyand Oncology Centre, Beijing Children’sHospital, Capital Medical University, Beijing, China.
7. Departmentof Paediatrics, Beijing Tongren Hospital, Capital Medical University, Beijing,China.
8. Departmentsof Ophthalmology & Vision Science, Hospital for Sick Children and Universityof Toronto, Toronto, Canada. Techna Institute, University Health Network,Toronto, Canada
Bothauthors contributed equally as first authors.
FinancialDisclosure(s): The author(s) have no proprietary or com-mercial interest in anymaterials discussed in this article.
HUMANSUBJECTS: Human subjects were included in this study. The ethical review boardapproved the study, with consideration to the tenets outlined in theDeclaration of Helsinki.
AuthorContributions:
Conceptionand design: Zhao, Gallie
Analysisand interpretation: Zhao, Gallie
Datacollection: Zhao, Li, Wu, L. Jin, Ma, M. Jin, Wang, Gallie
Obtainedfunding: none
Overallresponsibility: Zhao, Gallie
Correspondence:
BrendaGallie, MD, Department of Ophthalmology and Vision Science, Hospital for SickChildren, 555 University Avenue, Toronto, Ontario M5G1X8, Canada. E-mail: [email protected]
References
1.Munier FL, Soliman S, Moulin AP, et al. Profilingsafety of intravitreal injections for retinoblastoma using an anti-refluxprocedure and sterilisation of the needle track. Br J Ophthalmol.2012;96(8):1084-1087.
2.Francis JH, Brodie SE, Marr B, et al. Efficacyand toxicity of intravitreous chemotherapy for retinoblastoma: four-yearexpe-rience. Ophthalmology. 2017;124(4):488-495.
3. JiX-D, Lu S-L, Zhao P-Q. Vitrectomy for localized vitreous seeds ofretinoblastoma in an only eye. Chinese Med J. 2013;126:2589-2590.
4.Zhao J, Li S, Shi J, Wang N. Clinical presentation and group classificationof newly diagnosed intraocular retinoblastoma in China. Br J Ophthalmol.2011;95(10):1372-1375.
5.Mallipatna A, Gallie BL, Chévez-Barrios P, et al.Retino-blastoma. In: Amin MB, Edge SB, Greene FL, eds. AJCC Cancer StagingManual. 8th ed. New York: Springer; 2017: 819-831.
|
|





 发表于 2022-12-12 07:04:56
发表于 2022-12-12 07:04:56